

A teaching hospital is a university with surgical training programs and there are typically two surgeons on a case (surgery) working in tandem. A teacher surgeon is an attending (most senior) and a student surgeon is either a fellow or a resident (least senior). The C-SATS scoring system was built with the idea that there is only one surgeon performing at any given point in time even when there are two surgeon on a case. This worked well for robotic-assisted laparoscopic surgeries. However, as C-SATS expanded its footprint into teaching hospitals, the system was used more and more for non-robotic-assisted laparoscopic surgeries where surgeons worked in tandem. We heard from attendings at teaching hospitals that they wanted their individual scores separated out even though they are performing with fellow or resident in tandem. This posed major feasibility challenges but the bigger question is this: Why do attendings want to have individual scores on cases performed with another surgeon in tandem? To find out, I visited teaching hospitals, observed live surgeries in the O.R, and chatted with surgeons. To get employees to read the research findings, I created a “comic book” instead of writing a paper.
This case study is about a technical hurdle that prevented a design solution but I identified a new problem to solve that would give users and the business an even greater advantage.
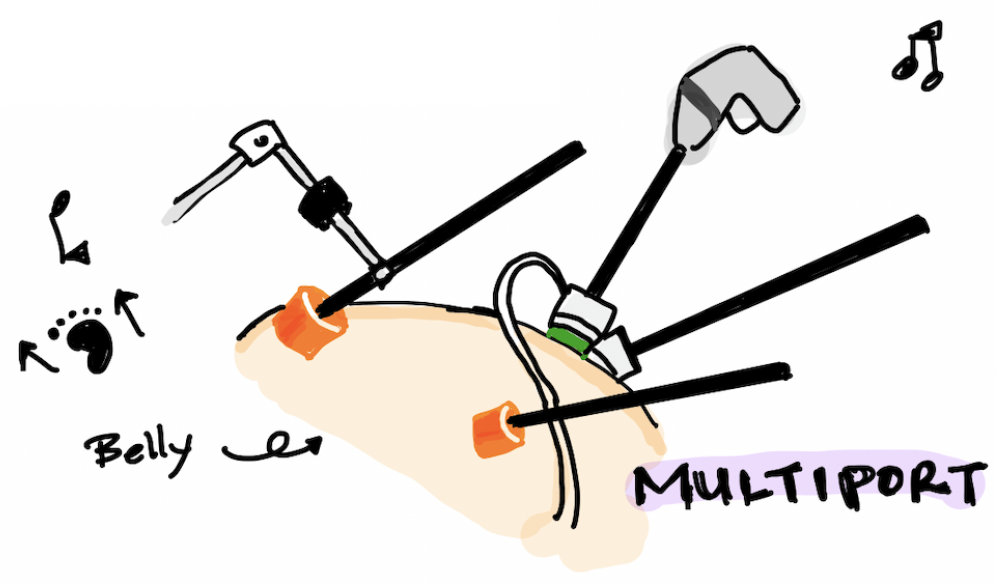
What is a Laparoscopic Surgery?
Laparoscopy is an operation performed in the abdomen or pelvis using small incisions with the aid of a camera. The laparoscope aids diagnosis or therapeutic interventions with a few small cuts in the abdomen. (Wikipedia)
The Nature of O.R. Orchestration
From the Medical Case Context project research, we know that nurses are the actual users of the C-SATS tablet. This applies to both non-teaching and teaching hospitals. During a procedure:
- Nurses are busy going in and out of the operating room (O.R.)
- It’s not always the same nurse that will use the tablet
- The C-SATS tablet is almost always placed in a hard to get to spot in the O.R. due to where it is allowed to plug into the power source
The operating rooms are often small with very limited tight space. C-SATS has a hardware component in the O.R., the tablet, that is used to record and upload videos. It has a recording screen that allows a toggle between surgeons to identify who performed during any segment of the surgery. In this example, the C-SATS tablet was attached to the power tower as seen in the bottom left corner of the room that had little to no foot traffic. For robotic surgeries, this feature was rarely used due to the nature of the O.R. orchestration and in the case of surgeries performed in tandem, it doesn’t really matter. Additionally, in order to correctly capture who is performing using the toggle feature meant that someone has to be dedicated to stand next to the tablet.
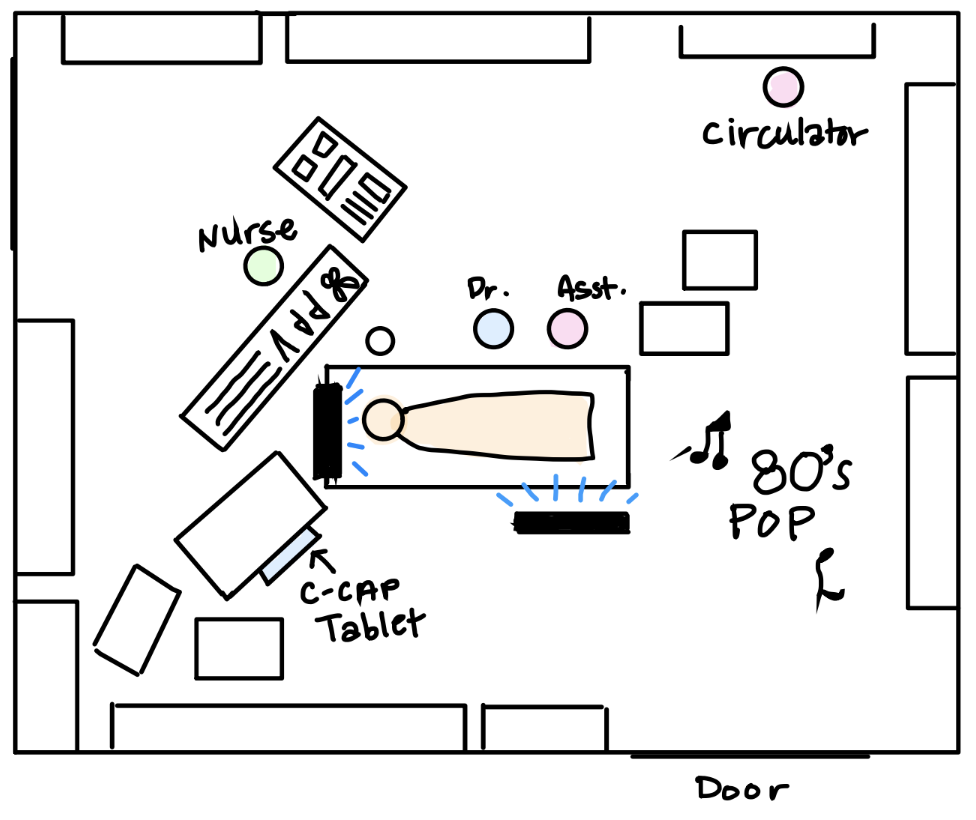
This second example is an uncommonly large O.R. The C-SATS tablet was hidden from view where I was sitting. It was attached to the power tower as seen in the bottom right corner of the sketch that had low foot traffic.

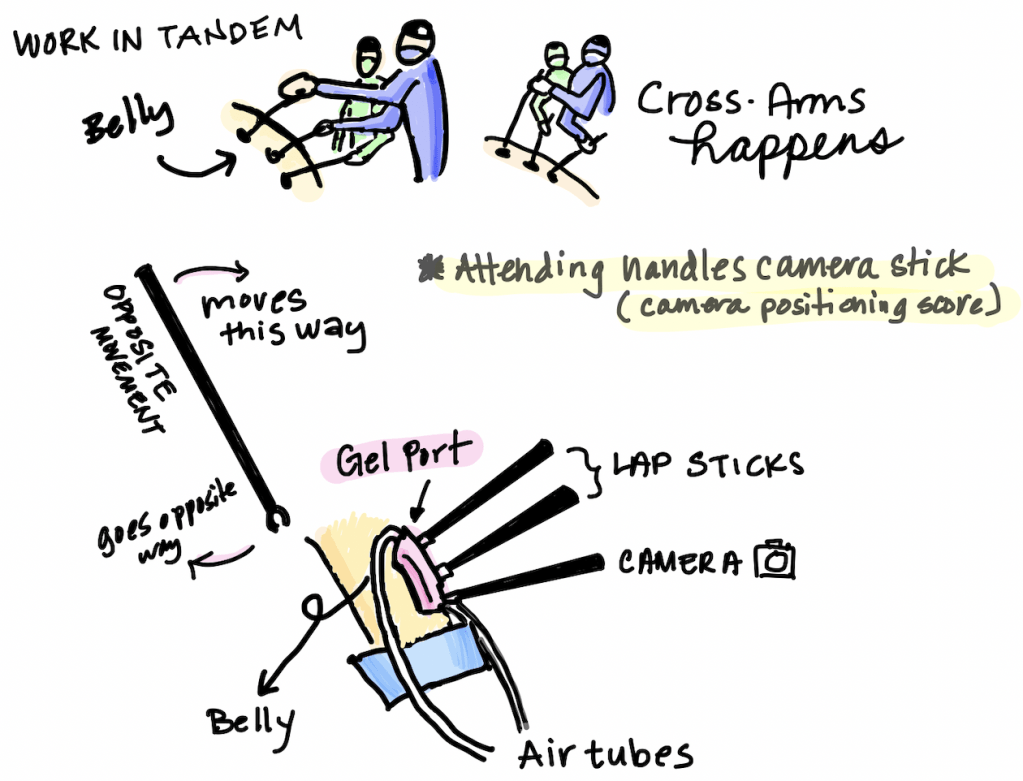
Always Work In Tandem
In teaching hospitals, surgeons worked side-by-side and performed at the same time. Sometimes the attending would put his/her hands over the fellow’s hands to guide him/her with the movements of the laparoscopes. C-SATS’s scoring system allows only one surgeon to be assigned to a segment of the surgery even though more than one surgeons performed at the same time.
Other Factors
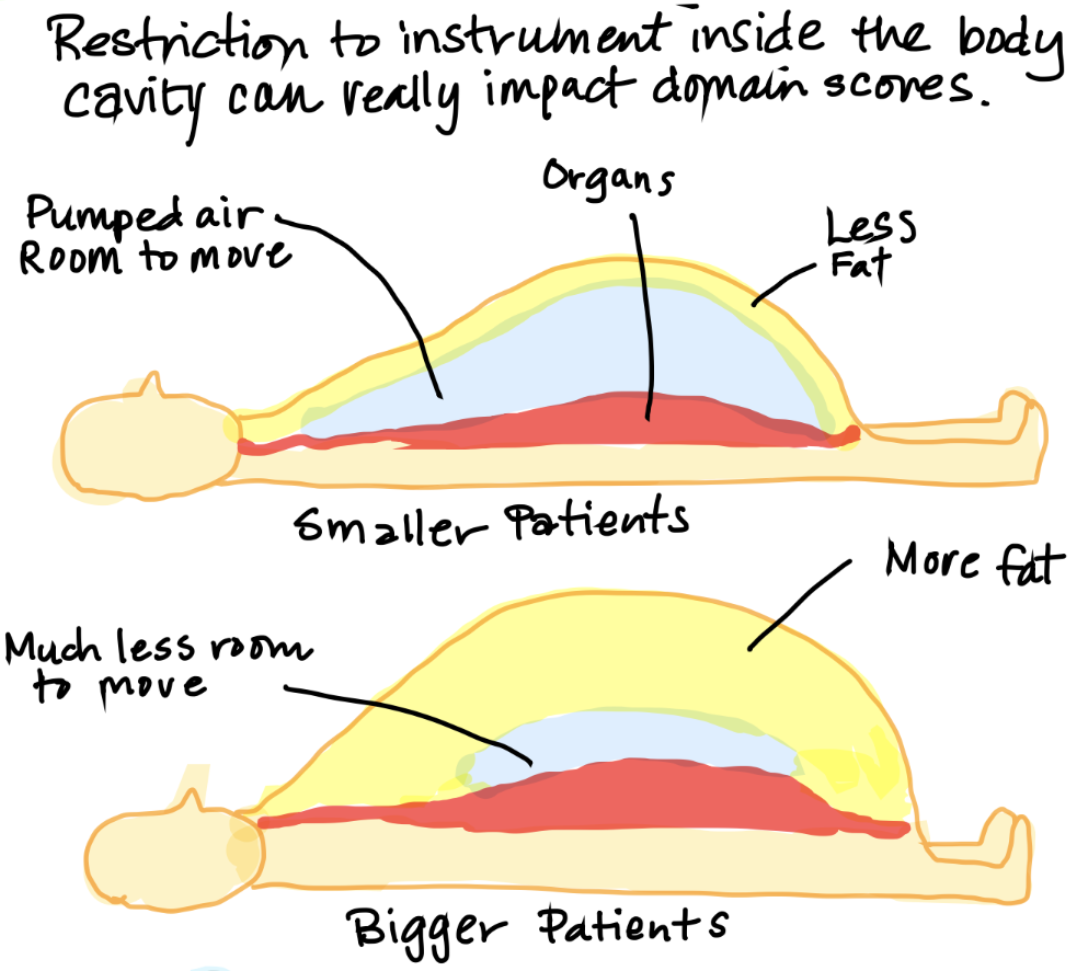
Low visibility into the belly cavity can cause reduction in efficiency and increase the time of a surgery.

The size of the patient can cause issues with visibility, camera placement, efficiency, force sensitivity, and bimanual dexterity. These are the surgical skills that are being evaluated. Sometimes surgeons have to pause the surgery and tilt the table and try different camera angles for better visibility. It also made some surgeons upset that these conditions weren’t being considered as a part of the review process.
The take aways from the research were:
- Lap surgeons in teaching hospitals work together in tandem
- Lap surgeons in teaching hospitals performed at the same time on the same surgery
- The C-SATS tablet is not easily accessible during recording
- The toggle feature won’t solve the scoring problem in teaching hospitals
- Even if only one surgeon performed by him/herself during a portion of the surgery, nurses aren’t always ready to use the toggle feature and change surgeon assignment
The Root of the Problem
Attendings are also users of the C-SATS system when they are not acting as teachers. When working with a less experienced surgeon, the score can be lower than an attending’s own performance scores. By assigning the team score to only the attending will negatively impact the attending’s individual scores. To change how C-SATS scoring system works meant a total rebuild of the system and it would be very expensive.
So Now What?
Without rebuilding the scoring system, there is no way to address clear score assignments for non-robotic-assisted laparoscopic surgeries in teaching hospitals. However, while I was out on my ethnographic tour, I interviewed attendings, fellows, and residents and asked them what makes a great surgeon in a teaching hospital. This was unanimous:

How Do We Measure Leadership Without a New Scoring System?
We know that:
- A surgeon is assigned a score for the segment of surgery that they performed
- We know the surgeons who paired on a case
- We know the teacher-student relationship between surgeons
- We know that a teacher has many students
- We know that a student has many teachers
I came up with the idea of team scores that allowed us to continue to use the existing scoring system to measure leadership. Instead of individual performance scores, there will be one shared case score. Teams that are strong would likely have good leadership and score consistently higher than teams with less leadership skills. Alternately, we can identify students who are struggling or excelling. This can be triangulated with more reviewed cases and we can even go back to older cases and pull data from there. At a high level, this is how it works:

At the end of the day, it is about patient outcomes whether a surgery was performed by an individual or a team of surgeons.
Note: We weren’t able to implement this concept because the business went a different direction.
